TV
viewing and cancer, the enemy in your front room, a television hypothesis
revisited, expanded and slightly revised.
By Dr Chris Barnes Bangor
Scientific and Educational Consultants March 2015. E-mail manager@bsec-wales.co.uk
Homepage for more cancer
research and all my other scientific work at
Abstract
The
notion of TV viewing and cancer is revisited. For the first time ever the
approximate cancer risk of using television transmitting and receiving
technologies is split into its two main component parts i.e. that of light at night hazard from
the TV screens and room lighting themselves
and that of Radio Frequency Emissions. With regard to radio frequency
emissions the risk for male and female hormonal cancers dominates the light
risk by a factor of approximately 3/2.
Both are discussed in terms of circadian disruption, melatonin
suppression and its effect on the body’s natural cancer protective/suppressive
systems. The overall relative risk of
developing a hormonal cancer in the 21st century is about 5 times
its value in 1947 when the enemy in your front room and TV emissions first
appeared.
Introduction
The
Cancer Research UK organisation has recently announced in a TV campaign that
despite more people surviving from
cancer than dying from it, overall incidence rates appear to be continuing to
rise.
When
a deeper analysis is made it is apparent that in recent years the incidence of
some cancers has actually fallen substantially.
Male lung cancer rates presenting perhaps the most obvious and explainable trend showing a decline some
10-15 years or so after the male peak in tobacco use. Female smoking lagged male smoking in
popularity and as a result the peak in female lung cancer has not long passed
us by.
Some
cancers, however, do indeed have overall incidence rates that would appear to
have been continuing to rise in Britain as far as historic statistics are
available even though I have recently shown that the same have already peaked/
saturated in the USA [1]. These would appear to be substantially the
male and female ‘hormonal’ cancers namely Prostate Cancer and Breast
Cancer.
Researchers
and epidemiologists too numerous to reference here, save a few examples, have
sought to explain increased incidence of all cancers and these types in general
in terms of causation by new or increasing environmental carcinogens.
Hallberg
and Johansson (2002) [2] concluded
there is a common environmental stress that accelerates several cancer forms
such as colon cancer, lung cancer, breast cancer, bladder cancer and malignant
melanoma. Further they stated that every effort should be taken to identify and
eliminate this stress. This present
paper aims to elucidate that said
stress in far more detail.
Some
have sought to explain increases in brain cancer and melanoma skin cancer in
terms of RF (radio frequency radiation), see Hallberg and Johansson (2011) [3].
They discuss RF radiation in terms of a weakening factor to the immune
system.
I
have previously sought to enquire
similarly if RF radiation is somehow a smoking gun when it comes to
cancer? I have considered UK statistics [4] and world statistics and geographic
distributions [5, 6].
The
conclusions I reached from my UK study [5]
were;
- Breast, prostate, leukaemia and brain cancers
were shown to be very closely correlated with each other and with the
growth of either TV receiver use and/or broadcasting of TV signals in the
period 1971-2002, but not with general per capita growth.
- The sum total of incidence of prostate and
breast cancer combined in the period 1947 to 2002 is extremely closely
correlated with the number of TV licenses issues in the UK R>.99. This
is suggestive of an extremely close association with TV receiver use
and/or the broadcasting of TV broadcast emissions.
- Use of polynomial expansion to predict cancer
incidence beyond 2010 suggests a long terms saturation for Leukaemia
incidence trend at circa 2005 and a fall thereafter, similar results are
obtained for breast cancer in the medium term with about a 6 year lag. This seems not inappropriate when
documented latency periods are taken into account.
- I proposed then that reasons for (3) above may
have been either due to the use of CRT TVS and monitors coming to an end
or the fact that many competing types of wireless technologies are
actually reducing risk.
One thing I didn’t consider at the time was the
effect of light emissions from TV screens or the fact that inherent in late night TV viewing is often
exposure to larger amounts of artificial light in the lounge or other rooms of
people’s houses nor did I consider the fact that daytime television viewing
would have caused more people to be indoors therefore depriving them of the
chance to acquire natural daylight and vitamin D.
As early as 1995, Web and Puig-Domingo (1995) first
pointed out that although many clinicians totally ignore melatonin status, it
interacts with and controls the metabolic activity of many endocrine and
non-endocrine tissues within the body [7].
It has been known from animal models since 2000
that all three pineal indoles increase the activity of superoxide dismutase and
lower the ratio of oxidized to reduced glutathione in the brain, see Liu and Ng
(2000) [8] . In other words Melatonin, 5MTT have powerful
antioxidant anti free radical properties.
At least from the lighting perspective Stevens and
Rea (2000) appear to concur with my present hypothesis.
Kos-Kudla (2002) [9] concluded that the presence of a negative correlation between
plasma melatonin and IGF-I concentrations in patients with neoplastic disease
implies the existence of an additional defence mechanism based on the
oncostatic influence of melatonin.
Sephton and Speigel (2003) [10] commented that emerging data in the human and animal
literature suggest that circadian regulation may be an important prerequisite
for the maintenance of host defences against cancer. Thus, stress-related
circadian disruption may have negative implications for cancer prognosis. Further their conclusion was that
psychosocial effects on cancer progression can be measured, and possibly
mediated, by the disruption of circadian function.
In 2005, Stevens (2005) [11] commented that global
impact of breast cancer is large and growing. Further was the comment that it
seemed clear that something about modern life was the culprit. Support has
developed for a possible role of “circadian disruption,” particularly from an
altered-lighted environment (such as light at night). Lighting during the night
of sufficient intensity can disrupt circadian rhythms, including reduction of
circulating melatonin levels and resetting of the circadian pacemaker of the
suprachiasmatic nuclei.
Reduced melatonin may increase breast cancer risk
through several mechanisms, including increased oestrogen production and
altered oestrogen receptor function. The genes that drive the circadian rhythm
are emerging as central players in gene regulation throughout the organism,
particularly for cell-cycle regulatory genes and the genes of apoptosis.
Aspects of modern life that can disrupt circadian rhythms during the key
developmental periods (e.g., in utero and during adolescence) may be
particularly harmful. Epidemiologic studies should consider gene and
environment interactions such as circadian gene variants and shift work requirements
on the job.
Melatonin has been experimentally
implicated in skin functions such as hair growth cycling, fur pigmentation, and
melanoma control, and melatonin receptors are expressed in several skin cells
including normal and malignant keratinocytes, melanocytes and has strong
antioxidant activity in U/V exposed skin cells, see Slominski et al 2005 [12].
Bartsch and Bartsch (2006) [13] have proposed that
melatonin disruption may be at least in part responsible the growing epidemic
of cancer, especially breast cancer in modern society.
Further Carillo-Vico et al (2006) [14]
show immunomodulatory role of melatonin, with regard to infection,
inflammation and autoimmunity and their evidence strengthens the notion that
the nature of an immune response may be modified, and therefore therapeutically
manipulated, by circadian effector signals.
Yet further in 2006 [15], Ross explains how melatonin
could play a role in
cancer treatment or even prevention
Alterations in melatonin receptor expression as
well as changes in endogenous melatonin production have been shown in circadian
rhythm sleep disorders, Alzheimer's and Parkinson's diseases, glaucoma,
depressive disorder, breast and prostate cancer, hepatoma and melanoma, see
Seithikurippu et al (2008) [16].
My expanded television hypothesis or at least a
part of it then becomes inherently simple.
Exposure to more light at night as a result of TV screens and the
attendant room lighting that goes with them significantly lowers individuals’
serum melatonin levels resulting in more cancers.
West
al (2011) [17] has shown that blue light as if from an LED
at 469nm is very potent at suppression melatonin and has an equivalent colour
temperature > 4000K.
TV screens and monitors have a colour
temperature of between 6500 and 9300K
and therefore represent a significant hazard for melatonin reduction and
hence and hence would be expected to be associated with increased risk of cancer for this reason
alone.
Even
as far back as 2004 Pauley (2004) [18]
comments
on how lighting has become a ‘public health issue’ and is particularly
concerned about the blue component in HID street lamps which have can have colour temperature of anywhere form 3000-20000K. The colour
temperature of TV screens and monitors is within this range and so they would
be expected to be equally dangerous but yet until this publication would appear
to have been given little, if any, attention.
Experimental
My
experimental analysis is based on readily available public domain data from a
number of sources including the BBC and Cancer Research UK.
I
have plotted historic cancer incidence for Breast and Prostate Cancer combined
against the number of TV Licenses issued so that the plot covers from 1947 to
the present day. See figure 1 below:
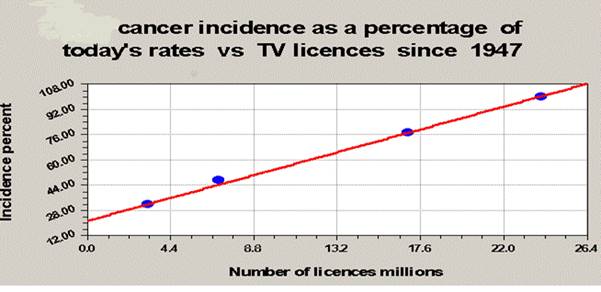
Figure
1: Incidence of ‘hormonal’ or endocrine sensitive cancers (sum of breast and
prostate) as a function of number of TV licences issued.
A
direct positive correlation with a Regression factor of > .99 is seen. The
two-tailed P value equals 0.0001 by all conventional criteria; this
difference is considered to be extremely statistically significant. The odds ratio for these two hormonal
cancers would appear to be of the order of 5 compared to before TV use was
common.
It
is instructive to see if cancer incidence due to this cause will saturate. Here
I am afraid I am at odds with CRCUK.
There latest projections say it will go on increasing. I say it should
saturate. In this respect saturation of TV’s per household is already seen and
Prostate Cancer in the UK would appear to be saturating likewise with a delay
due to latency and detection time. See figure 2 below:
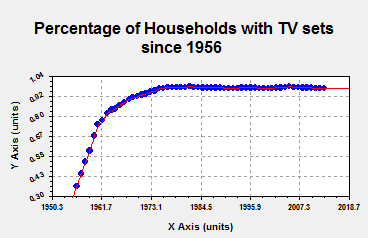

Figure
2: Saturation of TV penetration followed by saturation of prostate cancer
incidence some 20 years later.
This
is perhaps not surprising given that prostate cancer is known to have a long
latency period and can be dormant for up to 20 years before detection.
Results and Discussion.
The
experiential results strongly support the hypothesis that TV sets and attendant
lighting cause circadian and endocrine disruption which can lead to
cancer. That is not to say they are necessarily carcinogenic themselves but
simply that they disrupt the body’s natural protective system making it more
susceptible to oxidising free radicals, radiation and random mutations.
We
can also enquire if there are parallel dimensions at work here. Nothing in these findings is at odds with my
previous findings [4] because for
example as the number of TV sets has grown so has the number of transmitters.
I
have recently shown that RF emissions do appear to also have an association
with certain cancers. The so called ‘RF cancers’ [5]. I have further shown
that for a very small cohort in my local area all newly reported cases of
cancer I have heard of appear to have lived in residences exposed to more than
the average background of RF field strength [19]. One suggestion is
that this RF might simply act on the pineal gland rather in the same way that
light does. For example, Clark et al (2007) found among postmenopausal women,
increased residential RF exposures, transmitter proximity and visibility, and
temporally stable 60-Hz exposures were significantly associated with increased
E1G excretion. This association was strongest among postmenopausal women with
low overnight 6-OHMS levels [20].
Another
suggestion is that RF can generate free radicals in the body by disturbing
gas/liquid interfaces [21].
Another
suggestion is that certain modulation schemes can interfere with complex
molecular motions of the immune and cellular regenerative systems. With particular reference to the immune
system there is theoretical and experimental evidence that one should only
expect transient increases in cancer rates with the introduction of each type
of new technology. Such transients are
observed in figure 2 and have been discussed in more detail elsewhere, see
Lauer (2013) [22] and by the present author [23].
Besides
the above observations, I have also
noted a quantum mechanical effect of the effects of RF on both trees and people
which I have shown to be related to electromagnetic Aharonov Bohm effect which shows damage at
very specific distances from transmitting antennas and is related to
electromagnetic vector potential [24].
This parameter effectively carries information only i.e. the modulation
envelope of an RF emission. Since the
pineal gland has been shown to be magnetic field sensitive at ELF and modern modulation
envelopes carry ELF frequencies we have a good connection here. My theory is given good credence in the newly
released book Electromagnetic Fields in Biology and Medicine edited by Marko S.
Markov [25]. Such a phenomenon could under some circumstances
of demography produce either a hugely exaggerated risk or a hugely diminished
risk, not normally accounted for by epidemiologists. Sadly it would appear that the phenomenon is
true. This may also account why the
work of Cherry which takes into account TV transmitter antenna beam patterns
shows such an elevated risk for certain types of cancer [26].
Combining the risks
From
the above work it appears that TV sets their related light emissions, radio
waves, X ray emissions and ability to concentrate pollution and radon in
earlier CRT models only, have resulted in a cumulative odds ratio of circa 5. One would therefore expect the individual
risks for these components to all be
less than 5 but perhaps accumulate to that value or similar.
Megdal
et al 2005 suggest a relative risk of 1.51 for breast cancer and night shift
work [27] (i.e. exposure to light at night)
On
the other hand Hansen et al (2012) [28] suggest odds ratios as high as 2.8.
Conlon
et al 2007 suggest an odds ratio of 1.4 for shift work and prostate cancer [29].
Thus
an average estimate for both cancers is 1.9. It is reasonable and fair to assume that
the risk in exposing ourselves to bright Television screens and other household
lighting sources any time after about 8 o’clock at night which have a colour
temperature high enough to contain the blue wavelengths which can diminish
melatonin will be of the same order as those for night shift working.
Dolk
I (1996) found a relative risk of 1.83 for Leukaemia and skin cancer within 2
km of the Sutton Coldfield TV transmitter [30].
Wolf
and Wolf found an odds ratio of 4.15 for various cancers near a mobile phone
transmitter in Israel. This and other
statistics from around the world relating to RF exposure are to be found at http://apps.fcc.gov/ecfs/document/view?id=7520940908 [31].
The
average risk ratio taken from these two studies is 2.99.
Khurana
et al (2010) found that eight of the 10 studies reported increased prevalence
of adverse neurobehavioral symptoms or cancer in populations living at
distances < 500 meters from base stations [32]. None of the studies reported exposure above accepted
international guidelines, suggesting that current guidelines may be inadequate
in protecting the health of human populations.
Tuyn
et al (1985) considered the dose rate due to X-rays in the vicinity of TV and
VDU screens was determined using a xenon-filled proportional counter. The
results confirm that the X-ray dose rate around such devices is extremely low.
Of greater impact for the exposure of the population was found to be the
influence of the electrostatic field in the vicinity of a TV or VDU screen on
the local concentration of radon daughters. Such measurements were performed
using air sampling at various distances from the screens on a filter-surface
barrier detector unit to identify the radon daughters. The radon concentration
in the room was simultaneously measured using TLD in a device based on
electrostatic precipitation. It is shown that the presence of an electrostatic
field during operation of a TV or VDU screen reduces the radon daughter
concentration in its vicinity. In other words the result is counter to the
expected hypothesis. It is worthy of consideration, however, that when the device is switched off any
radon concentrated may leak back into the living space. Further Mahrok and Al-Dulamey (2005) showed variable emissions always less
than background radiation levels. [33].
Perhaps, therefore, for the purpose of the present estimation we can leave
radon out of the equation.
Thus
the cumulative average risk ratio in
relation to cancer when owning a TV set
and been exposed respectively to both
light and RF radiation is 1.9 + 2.99 = 4.98.
This is in remarkable agreement with my experimental
observation.
Moreover, I have shown that the TV set is truly an enemy
in your front room but that its light emission and attendant light exposure one
probably gets from other light in one’s lounge of other parts of the house equates to some 38% of the
total risk in using the technology.
The
rest comes from the all-pervasive RF radiation required to operate the
technology and at least in part its part on melatonin suppression for some
sections of society.
Finally, it is interesting to note
that Hallberg and Johansson remark on an explosion of melanoma skin cancer
after the 1950’s in Sweden and blame it on 90MHz FM broadcasting [34].
Of course TV transmission began in earnest about the same time and a new
enemy appeared in our living rooms. Melatonin
receptors are expressed in several skin cells including normal and malignant
keratinocytes, melanocytes and has strong antioxidant activity in U/V exposed
skin cells, see Slominski et al 2005 [35]. Thus light exposure from TV sets and
attendant household lighting could be having a similar effect on melanoma rate
as for hormonal cancer rates.
It
would seem there is a strong case for introducing all cable technology using
either copper or fibre to deliver our TV transmissions to our homes. Further it would appear the best time to
watch television is in the morning thereby boosting serotonin rather than at
night diminishing melatonin as many and most of us do.
Conclusions
·
The
sum total of incidence of prostate and breast cancer combined in the period
1947 to 2002 is extremely closely correlated with the number of TV licenses
issues in the UK R>.99. P= 0.0001. This
is suggestive of an extremely
close association
with TV receiver use and/or the broadcasting of TV broadcast emissions.
·
For
the 1st time ever a scientific paper has separated out the risks of using
Television broadcasting (the enemy in your home) into relative components.
·
Exposure
to radio frequency energy would still appear to pose a larger risk than that
form exposure to light form the TV screen and attendant household lighting
itself but this latter risk is far from insignificant.
·
In
TV broadcasting some 62% of the cancer risk come from exposure to RF radiation
·
Whereas
38% most likely come from exposure to light from the TV screen and other
associated household and external ‘light at night sources.’
·
Use
of TV broadcasting and receiving technology
in its present form poses a risk for hormonal cancers such as breast and
prostate some 5 times greater than if it were not present i.e. compared to and calculated from pre-TV era cancer
incidence figures.
·
The
analysis here is suggestive that hormonal/RF/endocrine/Cancer rates will not continue to rise indefinitely as
seen in the recent CRC UK website projections and TV advertising campaign but
will, in fact, saturate at more or less
present day levels as they have done in the USA. If some RF and LAN ( light at night ) can be
removed we may even be able to significantly reduce these rates.
References
1.
http://www.drchrisbarnes.co.uk/UKTesting%20.html
2.
http://search.informit.com.au/documentSummary;dn=542505625986648;res=IELHEA
3.
http://www.pathophysiologyjournal.com/article/S0928-4680%2811%2900027-7/abstract,
4.
http://www.drchrisbarnes.co.uk/Meta.html
5.
http://www.drchrisbarnes.co.uk/World.htm
6.
http://drchrisbarnes.co.uk/CAGIS.htm
7.
http://www.researchgate.net/publication/15441419_Role_of_melatonin_in_health_and_disease
8.
http://www.nrcresearchpress.com/doi/abs/10.1139/o00-018#.VPNzG471Zkg.
9.
http://forum.annalsoftransplantation.com/abstract/index/idArt/420807/act/3
10. http://www.sciencedirect.com/science/article/pii/S0889159103000783
11. http://www.ncbi.nlm.nih.gov/pubmed/15703542
12. http://link.springer.com/article/10.1385/ENDO:27:2:137#page-1
13. http://www.impactaging.com/papers/v2/n2/full/100126.html
14. http://www.ncbi.nlm.nih.gov/pubmed/16729718
15. http://jnci.oxfordjournals.org/content/98/12/806.short
16. http://www.sciencedirect.com/science/article/pii/S0301008208000348.
17. http://jap.physiology.org/content/110/3/619
18. http://www.ncbi.nlm.nih.gov/pubmed/15325001
19. http://www.drchrisbarnes.co.uk/CancerHouses.htm
20. http://www.ncbi.nlm.nih.gov/pubmed/18000420
21. http://www.drchrisbarnes.co.uk/Unified.htm
22. https://hal.archives-ouvertes.fr/file/index/docid/877298/filename/publiarx.pdf
23. http://www.drchrisbarnes.co.uk/UKTesting%20.html.
24. http://drchrisbarnes.co.uk/More%20egg%20than%20chicken.html
25. http://www.crcpress.com/product/isbn/9781482248500
26. https://researcharchive.lincoln.ac.nz/bitstream/10182/3969/1/90_r3_EMR_Sutro_Paper_09-02%5Bpdf
27. http://www.ncbi.nlm.nih.gov/pubmed/16084719
28. http://www.sciencedirect.com/science/article/pii/S0959804911005016
31. http://apps.fcc.gov/ecfs/document/view?id=7520940908
32. http://www.brain-surgery.us/Khurana_et_al_IJOEH-Base_Station_RV.pdf
33. http://www.iasj.net/iasj?func=fulltext&aId=43382
34. http://avaate.org/IMG/pdf/melanoma_fm.pdf
35. http://link.springer.com/article/10.1385/ENDO:27:2:137#page-1